Erectile Dysfunction From Biological Processes Standpoint
Erectile dysfunction stands for inability to achieve stable and maintainable erection sufficient to conduct a sexual intercourse. This term recently replaced a less accurate classification of ‘impotence’, together with the identification of the prevalence of this disease, the discovery of the key molecular mechanisms of its pathogenesis and the emergence of new and effective means of pharmacological correction. According to population-based studies carried out in North and South America, Asia and Europe, the incidence of erectile dysfunction in adult males is ranging from 15 to 50%, with approximately 10% of cases of severe dysfunction.
The physiological mechanism of erection
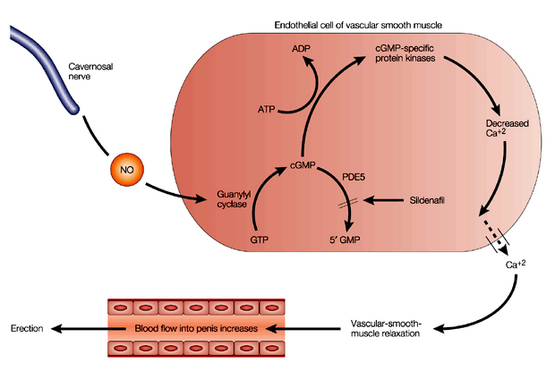
Psychogenic erectile dysfunction is preceded by reflex stimulation. It is transmitted from the brain along the pathways in the spinal cord and then to the cavernous nerve endings in the walls of arteries and branches of the same name in the trabeculae of the cavernous bodies of the penis. Part of the cavernous nerve fibers are neither adrenergic nor cholinergic-mediated, their mediator is nitric oxide (NO). When a neuro-mediator is secreted, NO penetrates the membrane of smooth muscle cells and activates guanylate cyclase in them, resulting in increased production of cyclic guanosine monophosphate (cGMP). As a result of a cascade of biochemical transformational the changes in permeability of calcium and potassium channels take place. The concentration of potassium inside smooth muscle cells increases and calcium concentration decreases, and the smooth muscles of the penis cells relax.
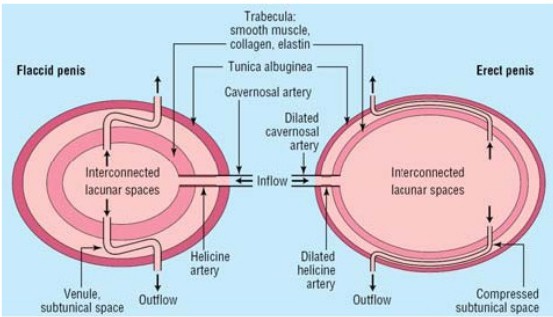
Relaxation of smooth muscle walls of the cavernous arteries is an extension of the inner lumen, which increases blood flow. Relaxation of smooth muscles of the trabecular corpus cavernosum leads to an increase in volume, as well as compression of draining veins, preventing the outflow of blood from the cavernous bodies. Thus, the penis fills with blood, expands and erection is achieved.
Increasing and maintaining erection is possible due to the inclusion of additional reserves. Increased blood flow in the penis accompanied by activation of usually dormant arteries. Increase of endothelial blood flow and dilation of endothelial cells lining the trabeculae of the cavernous bodies (corpora cavernosa) leads to an increased release of NO from those cells. In this case, NO acts as a local hormone. Its paracrine effect arising through the molecular mechanisms described above (with cGMP) promotes additional relaxation of the trabecular smooth muscles of cavernous bodies and the arteries themselves. This ensures that erection is maximized.
Many biologically active substances, both mediators and modulators, provide or regulate the process of erection at the central and peripheral levels. Yet a key role in the emergence, achievement and maintenance of erection is a result of increased NO secretion.
A coordination with the effect of NO-ergic mechanisms involved in the regulation of erectile function cholinergic and adrenergic components of the autonomic nervous system plays a vital role. Stimulation of M2,3-cholinergic nerves endings and atypical (Ps) adrenoceptor blockade of a2-adrenergic receptors is caused by the modulation of tone in the CNS or local mechanisms by increasing cGMP production promotes relaxation of smooth muscle tissue cavity.
Molecular mechanism of suppression of erection is no longer an area unknown. It relates to the enzymatic cleavage of cGMP phosphodiesterase (PDE). This enzyme has many specific and different types of tissues and organs. The tissue of cavernous bodies is represented, mainly, by the fifth type of PDE (PDE-5); the element of regulation was recently the object of a successful pharmacological interventions to correct erectile dysfunction.
Causes of Erectile dysfunction

The possible causes of ED are diverse: ageing, mental and neurological disorders, endocrine and somatic disease, illness or injury of the genitals, side effects of certain medicines. Once it was assumed that in most cases, impotence has a psychogenic nature. However, a group of experts of National Institutes of Health in far 1993 concluded that in most cases (about 75%) ED problems are caused by vascular lesions. Epidemiological studies carried out in recent years have clarified that the incidence of ED in the population, especially among middle-aged men in the majority of cases is associated with a variety of risk factors, often combined and interconnected, which include aging, diabetes mellitus, atherosclerosis, arterial hypertension, obesity, smoking, alcohol abuse, sedentary lifestyle, mental depression and a relatively low level of education.
It is obvious that almost all of the above factors (including depression) at the same time represent risk factors for cardiovascular diseases and mortality. It is therefore not surprising that the presence of cardiovascular disease (CVD) is a very important risk factor for ED. In a large multicenter epidemiological Men’s Health Study research, it was found that in the presence of CVD the likelihood of ED increases almost by 3 times with a significant prevalence of moderate to severe dysfunction. There is also evidence of an inverse relationship that allows considering that ED as a possible harbinger of hidden flowing vascular heart disease and hypertension.
Why are multiple and diverse risk factors contribute to the parallel development of diseases of the cardiovascular system and the ED? A rational explanation for this is the existence of dependent risk factors of common pathogenetic mechanisms, such as the breakdown and disintegration of the autonomic nervous system, metabolic syndrome, endothelial dysfunction that cause dysregulation of vascular tone, and then the structure of the blood vessels (heart, brain, penis, and so on. d.).
A large and universal significance in the genesis of CVD and ED has recently attached to the phenomenon of endothelial dysfunction. It is expressed in the loss of their regulatory properties, primarily the ability to modulate the tone bordering on the endothelium of smooth muscle due to lower local NO products. The development of this phenomenon is implicated by the majority of the above risk factors.
Erectile Dysfunction as a side effect of medicines
Following the most important commandments of doctors ‘Don’t panic!’, you need to consider the possibility that ED may be provoked by the meds you take. Used for the prevention and treatment of cardiovascular disease. This primarily thiazide diuretics and other drugs, p-blockers, centrally acting antihypertensive agents (clonidine) and lipid lowering drugs (statins and fibrates), some psychotropic drugs, and possibly ACE inhibitors. On the contrary, favorable in this respect are a-blockers, and possibly angiotensin receptor antagonists, while the neutral ones are antagonists of slow calcium channels. It is obvious that in view of these facts, physicians should seek to avoid unnecessary use of appropriate medications and select the dose carefully.
However, there is a risk of inducing anxiety in patients. A series of studies proves that information (warning) about the possibility of ED patients with the use of drugs (such as beta-blockers) often causes anxiety and a secondary (psychogenic) ED. Therefore, to identify possible adverse effects is required, but it should be done deliberately and delicately.
Related:
http://www.mycanadianpharmacyrx.com/how-to-maintain-the-good-erection-for-as-long-as-possible.html
PDH-5 inhibitors – new means of pharmacological ED correction
Drugs of this class have a common mechanism of action. They selectively block the destruction of cGMP caused by PDH-5, and address the NO deficit. NO is necessary to cause and maintain an erection sufficiently long for an intercourse to take place. The chemical structure, pharmacological activity, selectivity, pharmacokinetic characteristics of different drugs. A wide range of preparations – Levitra, Canadian Cialis, Generic Viagra and dozens of their generic modifications demonstrate the results that are second to none. A considerable impact is observed in 64% of cases, while at least minor improvements are reported in 82% of treatment cases. The price range for original drugs starts from $15-20 per pill, although you may considerably decrease your expenses without any quality loss – drop in at My Canadian Pharmacy website for more information.









